SUBHEAD: Review of the TSA X-ray backscatter body scanner safety report: hide your kids, hide your wife.
By Jason Bell on 22 November 2010 in My Helical Tryst -
(http://myhelicaltryst.blogspot.com/2010/11/tsa-x-ray-backscatter-body-scanner.html)
Image above: This X-ray pin-up girl is just pixels. Not so TSA victims. From (http://www.wired.com/rawfile/2010/09/x-ray-pin-up-girls-are-just-pixels).
 Quite some time ago, I posted a short educational video that describes how BRCA1 and BRCA2 mutations cause cancer. In short, when a person who has a mutation in one of these genes is exposed to environmental factors that cause DNA damage, they simply don't repair the damage with the same efficiency as the general population.
Quite some time ago, I posted a short educational video that describes how BRCA1 and BRCA2 mutations cause cancer. In short, when a person who has a mutation in one of these genes is exposed to environmental factors that cause DNA damage, they simply don't repair the damage with the same efficiency as the general population.
Over the course of their lifetime, the incremental exposures to relative small and seemingly safe doses of ionizing radiation (which is everything from UV light to X-rays to gamma radiation) statistically accumulate damage (or the effects of damage and improper repair) until the probability of developing cancer becomes almost certain.
This is because BRCA1 and BRCA2 are both part of a molecular process that is very similar to the spell-check on your word processor (in oncology parlance, these genes are known as caretakers of the genome for this specific reason). When these genes don't work, mutations accumulate faster and eventually results in cancer. Its because of my interest in this aspect of cancer biology that I felt compelled to review the safety reports released on the TSA website here.
However, my interest is not only professional, but also personal. My grandmother died of breast cancer in 2005 after being in remission for 20+ years. While she was never tested for either BRCA1 or BRCA2, her family history indicates that there is a strong probability of one of these mutations running in my family. Including my grandmother, at least four of her siblings developed cancer: two died of breast cancer, one developed a rare form of leukemia and another died of skin cancer. All of her female siblings had cancer, and its noteworthy that her mother died of a very young age (maybe 30's or early 40's) of an unknown (to me) cause.
For these reasons, I fear that inadequate safety evaluation of these machines could unduly expose my family (and myself) to levels of radiation that might be harmful should this high familial cancer rate in fact be hereditary. Last spring, a group of scientists at the University of California at San Francisco (UCSF) including John Sedat Ph.D., David Agard Ph.D., Robert Stroud, Ph.D. and Marc Shuman, M.D. sent a letter of concern to the TSA regarding the implementation of their 'Advanced Imaging Technology', or body scanners as a routine method of security screening in US airports. Of specific concern is the scanner that uses X-ray back-scattering. In the letter they raise some interesting points, which I've quoted below:
The TSA has been stating that the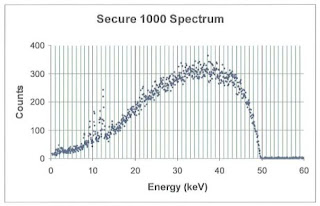 X-rays used in the back scatter machines use 'soft' X-rays, which are defined as radiation between 0.12-12 keV (or kilo electron volts) and are generally stopped, or absorbed, by soft tissue or low density matter. 'Hard' X-rays are between 12-128 keV and are absorbed by dense matter like bone. According to the TSA safety documents, AIT uses an 50 keV source that emits a broad spectra (see adjacent graph from here).
X-rays used in the back scatter machines use 'soft' X-rays, which are defined as radiation between 0.12-12 keV (or kilo electron volts) and are generally stopped, or absorbed, by soft tissue or low density matter. 'Hard' X-rays are between 12-128 keV and are absorbed by dense matter like bone. According to the TSA safety documents, AIT uses an 50 keV source that emits a broad spectra (see adjacent graph from here).
Essentially, this means that the X-ray source used in the Rapiscan system is the same as those used for mammograms and some dental X-rays, and uses BOTH 'soft' and 'hard' X-rays.
Its very disturbing that the TSA has been misleading on this point. Here is the real catch: the softer the X-ray, the more its absorbed by the body, and the higher the biologically relevant dose! This means, that this radiation is potentially worse than an a higher energy medical chest X-ray. With that being said, because the scanners have both a radiation source AND a detector in the front AND back of the person in the scanner, it is actually possible for the hardware to conduct a classic, through-the-body X-ray.
The TSA claims that the machines are not currently being used in that way; however, based on the limited engineering schematics released in the safety documents, they could be certainly be easily reconfigured to do so by altering the aluminum-plate (or equivalent) filter or by changing the software. So the hardware has the capability to output quite high doses of radiation, however a biological dose is a function of the time of exposure as well as the proximity to the source and the power of the power of the source.
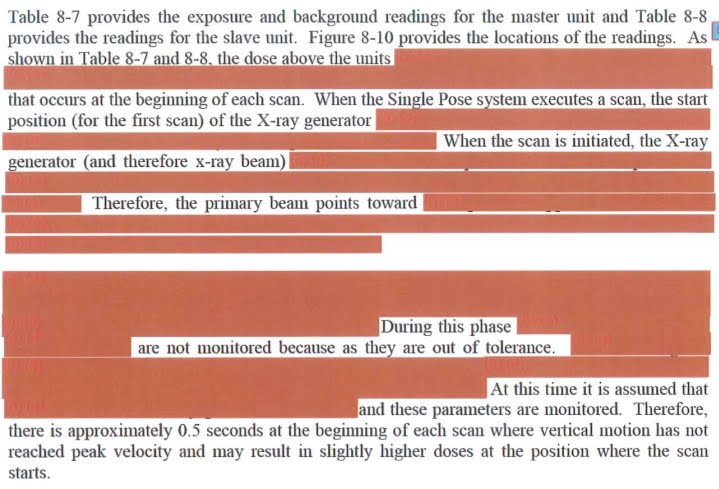
Unfortunately, it is difficult to determine which zones in the scanner are 'hottest' because that information is masked in the document. An excerpt of the safety evaluation from Johns Hopkins is shown below to give you sense of how much other information is being withheld. Ultimately my point is this: even though the dose may actually be low, these machines are capable of much higher radiation output through device failure or both unauthorized or authorized reconfiguration of either hardware or software.
 Which brings me to how the scanner works. Essentially, it appears that an X-ray beam is rastered across the body, which highlights the importance of one of the specific concerns raised by the UCSF scientists... what happens if the machine fails, or gets stuck, during a raster. How much radiation would a person's eye, hand, testicle, stomach, etc be exposed to during such a failure.
Which brings me to how the scanner works. Essentially, it appears that an X-ray beam is rastered across the body, which highlights the importance of one of the specific concerns raised by the UCSF scientists... what happens if the machine fails, or gets stuck, during a raster. How much radiation would a person's eye, hand, testicle, stomach, etc be exposed to during such a failure.
What is the failure rate of these machines?
What is the failure rate in an operational environment?
Who services the machine? What is the decay rate of the filter?
What is the decay rate of the shielding material?
What is the variability in the power of the X-ray source during the manufacturing process?
This last question may seem trivial; however, the Johns Hopkins Applied Physics Laboratory noted significant differences in their test models, which were supposed to be precisely up to spec.
It's also interesting to note that the Johns Hopkins Applied Physics Laboratory criticized other reports from NIST (the National Institute of Standards and Technology) and a group called Medical and Health Physics Consulting for testing the machine while one of the two X-ray sources was disabled (citations at the bottom of the page). These questions have not been answered to any satisfaction and the UCSF scientists, all esteemed in their fields and members of the National Academy of Sciences have been dismissed based on a couple of reports seemingly hastily put together by mid-level government lab technicians.
The documents that I have reviewed thus far either have NO AUTHOR CREDITS or are NOT authored by anyone with either a Ph.D. or a M.D., raising serious concerns of the extent of the expertise of the individuals and organizations evaluating these machines. Yet, the FDA and TSA continue to dismiss some of the most talented scientists in the country...
With respect to errors in the safety reports and/or misleading information about them, the statement that one scan is equivalent to 2-3 minutes of your flight is VERY misleading. Most cosmic radiation is composed of high energy particles that passes right through our body, the plane and even most of the earth itself without being absorbed or even detected. The spectrum that is dangerous is known as ionizing radiation and most of that is absorbed by the hull of the airplane. So relating non-absorbing cosmic radiation to tissue absorbing man-made radiation is simply misleading and wrong.
Furthermore, when making this comparison, the TSA and FDA are calculating that the dose is absorbed throughout the body. According the simulations performed by NIST, the relative absorption of the radiation is ~20-35-fold higher in the skin, breast, testes and thymus than the brain, or 7-12-fold higher than bone marrow. So a total body dose is misleading, because there is differential absorption in some tissues.
Of particular concern is radiation exposure to the testes, which could result in infertility or birth defects, and breasts for women who might carry a BRCA1 or BRCA2 mutation. Even more alarming is that because the radiation energy is the same for all adults, children or infants, the relative absorbed dose is twice as high for small children and infants because they have a smaller body mass (both total and tissue specific) to distribute the dose. Alarmingly, the radiation dose to an infant's testes and skeleton is 60-fold higher than the absorbed dose to an adult brain!
There also appears to be unit conversion error in the Appendix of the report, which was recently cited by the FDA in response to the UCSF scientist's letter of concern, which might mean that the relative skin dose is 1000-fold higher than the report indicates (pg Appendix B, pg ii, units of microSv are used in an example calculation, when it appears that units of milliSv should have been used).
I attempted to contact the author, Frank Cerra, to query whether this was a computational mistake or an unexplained conversion; however, none of his web-published email addresses are valid and there was no answer by phone. I cannot rule out that a conversion factor was used that was not described in the methods, and would welcome confirmation or rebuttal of this observation.
Finally, I would like to comment on the safety of the TSA officers (TSO) who will be operating these machines, and will be constant 'bystanders' with respect to the radiation exposure. The range of exposure estimates is a function of where an officer stands during their duty, what percentage of that duty is spent in the same location and how often the machine is running. A TSO could be exposed to as much as 86-1408 mrem per year (assuming 8 hours per day, 40 hours a week, 50 weeks per year and between 30-100% duty and 25-100% occupancy, as defined by the Johns Hopkins report), which is between 86%-1410% of the safe exposure of 100 mrem.
At the high end, if for example a TSO is standing at the entrance of the scanner when it is running at maximum capacity, then that officer could hit their radiation exposure limit in as few as 20 working days (assuming an 8 hour shift). While we may not be very happy with our TSOs at the moment as the face of these policies, we need to keep in mind that they really should be wearing radiation badges in order to know their specific exposure (especially for those officers who may also have to receive radiation exposure for medical reasons).
As far as I'm concerned, the jury is still out on whether these machines are safe or even could be made safe for this application. Until then, I suggest keeping your family out of these machines and as vile as it is, either submit to a physical search or just don't fly. Safety reports that should be considered invalid due to the fact that one of the two X-ray sources was disabled during testing:
 Jason Bell, "a molecular biologist and biophysicist... a Ph.D. candidate in Steve Kowalczykowski's lab at UC Davis," has posted a detailed critique of the research on the safety of airport backscatter radiation scanners. His specialty is the "molecular mechanism of how mutations in the breast cancer susceptibility gene, BRCA2, result in cancer," and he's posted a detailed, lay-friendly explanation of the scientific concerns expressed by the UCSF team that believes that they are unsafe for use.
Jason Bell, "a molecular biologist and biophysicist... a Ph.D. candidate in Steve Kowalczykowski's lab at UC Davis," has posted a detailed critique of the research on the safety of airport backscatter radiation scanners. His specialty is the "molecular mechanism of how mutations in the breast cancer susceptibility gene, BRCA2, result in cancer," and he's posted a detailed, lay-friendly explanation of the scientific concerns expressed by the UCSF team that believes that they are unsafe for use.
By Jason Bell on 22 November 2010 in My Helical Tryst -
(http://myhelicaltryst.blogspot.com/2010/11/tsa-x-ray-backscatter-body-scanner.html)
Image above: This X-ray pin-up girl is just pixels. Not so TSA victims. From (http://www.wired.com/rawfile/2010/09/x-ray-pin-up-girls-are-just-pixels).
[IB Editor's note: We were informed, by Garrett Spaulding, on 5/4/12 that the blog that this article originally was linked to has been removed by its author. Garrett has written a thoughtful piece on the subject here (http://www.travelinsurance.org/tsas-body-scanner-technology-health-risks/)]
I am a biochemist working in the field of biophysics. Specifically, the lab I work in (as well as many others) has spent the better part of the last decade working on the molecular mechanism of how mutations in the breast cancer susceptibility gene, BRCA2, result in cancer.
The result of that work is that we now better understand that people who have a deficient BRCA2 gene are hypersensitive to DNA damage, which can be caused by a number of factors including: UV exposure, oxidative stress, improper chromosomal replication and segregation, and radiation exposure. The image below shows what happens to a chromosome of a normal cell when it is exposed to radiation. It most cases, this damage is repaired; however, at high doses or when there is a genetic defect, the cells either die or become cancerous.
The result of that work is that we now better understand that people who have a deficient BRCA2 gene are hypersensitive to DNA damage, which can be caused by a number of factors including: UV exposure, oxidative stress, improper chromosomal replication and segregation, and radiation exposure. The image below shows what happens to a chromosome of a normal cell when it is exposed to radiation. It most cases, this damage is repaired; however, at high doses or when there is a genetic defect, the cells either die or become cancerous.
Quite some time ago, I posted a short educational video that describes how BRCA1 and BRCA2 mutations cause cancer. In short, when a person who has a mutation in one of these genes is exposed to environmental factors that cause DNA damage, they simply don't repair the damage with the same efficiency as the general population.Over the course of their lifetime, the incremental exposures to relative small and seemingly safe doses of ionizing radiation (which is everything from UV light to X-rays to gamma radiation) statistically accumulate damage (or the effects of damage and improper repair) until the probability of developing cancer becomes almost certain.
This is because BRCA1 and BRCA2 are both part of a molecular process that is very similar to the spell-check on your word processor (in oncology parlance, these genes are known as caretakers of the genome for this specific reason). When these genes don't work, mutations accumulate faster and eventually results in cancer. Its because of my interest in this aspect of cancer biology that I felt compelled to review the safety reports released on the TSA website here.
However, my interest is not only professional, but also personal. My grandmother died of breast cancer in 2005 after being in remission for 20+ years. While she was never tested for either BRCA1 or BRCA2, her family history indicates that there is a strong probability of one of these mutations running in my family. Including my grandmother, at least four of her siblings developed cancer: two died of breast cancer, one developed a rare form of leukemia and another died of skin cancer. All of her female siblings had cancer, and its noteworthy that her mother died of a very young age (maybe 30's or early 40's) of an unknown (to me) cause.
For these reasons, I fear that inadequate safety evaluation of these machines could unduly expose my family (and myself) to levels of radiation that might be harmful should this high familial cancer rate in fact be hereditary. Last spring, a group of scientists at the University of California at San Francisco (UCSF) including John Sedat Ph.D., David Agard Ph.D., Robert Stroud, Ph.D. and Marc Shuman, M.D. sent a letter of concern to the TSA regarding the implementation of their 'Advanced Imaging Technology', or body scanners as a routine method of security screening in US airports. Of specific concern is the scanner that uses X-ray back-scattering. In the letter they raise some interesting points, which I've quoted below:
- "Our overriding concern is the extent to which the safety of this scanning device has been adequately demonstrated. This can only be determined by a meeting of an impartial panel of experts that would include medical physicists and radiation biologists at which all of the available relevant data is reviewed."
- "The X-ray dose from these devices has often been compared in the media to the cosmic ray exposure inherent to airplane travel or that of a chest X-ray. However, this comparison is very misleading: both the air travel cosmic ray exposure and chest X-rays have much higher X-ray energies and the health consequences are appropriately understood in terms of the whole body volume dose. In contrast, these new airport scanners are largely depositing their energy into the skin and immediately adjacent tissue, and since this is such a small fraction of body weight/vol, possibly by one to two orders of magnitude, the real dose to the skin is now high."
- "In addition, it appears that real independent safety data do not exist."
- "There is good reason to believe that these scanners will increase the risk of cancer to children and other vulnerable populations. We are unanimous in believing that the potential health consequences need to be rigorously studied before these scanners are adopted."
In order to really understand these concerns, I think its important to consider the type of radiation used in these scanners, which the TSA has described as 'soft' and 'safe'. First, we need to clarify the definition of 'soft' vs 'hard' X-rays.
The TSA has been stating that the
 X-rays used in the back scatter machines use 'soft' X-rays, which are defined as radiation between 0.12-12 keV (or kilo electron volts) and are generally stopped, or absorbed, by soft tissue or low density matter. 'Hard' X-rays are between 12-128 keV and are absorbed by dense matter like bone. According to the TSA safety documents, AIT uses an 50 keV source that emits a broad spectra (see adjacent graph from here).
X-rays used in the back scatter machines use 'soft' X-rays, which are defined as radiation between 0.12-12 keV (or kilo electron volts) and are generally stopped, or absorbed, by soft tissue or low density matter. 'Hard' X-rays are between 12-128 keV and are absorbed by dense matter like bone. According to the TSA safety documents, AIT uses an 50 keV source that emits a broad spectra (see adjacent graph from here).Essentially, this means that the X-ray source used in the Rapiscan system is the same as those used for mammograms and some dental X-rays, and uses BOTH 'soft' and 'hard' X-rays.
Its very disturbing that the TSA has been misleading on this point. Here is the real catch: the softer the X-ray, the more its absorbed by the body, and the higher the biologically relevant dose! This means, that this radiation is potentially worse than an a higher energy medical chest X-ray. With that being said, because the scanners have both a radiation source AND a detector in the front AND back of the person in the scanner, it is actually possible for the hardware to conduct a classic, through-the-body X-ray.
The TSA claims that the machines are not currently being used in that way; however, based on the limited engineering schematics released in the safety documents, they could be certainly be easily reconfigured to do so by altering the aluminum-plate (or equivalent) filter or by changing the software. So the hardware has the capability to output quite high doses of radiation, however a biological dose is a function of the time of exposure as well as the proximity to the source and the power of the power of the source.
Unfortunately, it is difficult to determine which zones in the scanner are 'hottest' because that information is masked in the document. An excerpt of the safety evaluation from Johns Hopkins is shown below to give you sense of how much other information is being withheld. Ultimately my point is this: even though the dose may actually be low, these machines are capable of much higher radiation output through device failure or both unauthorized or authorized reconfiguration of either hardware or software.
 Which brings me to how the scanner works. Essentially, it appears that an X-ray beam is rastered across the body, which highlights the importance of one of the specific concerns raised by the UCSF scientists... what happens if the machine fails, or gets stuck, during a raster. How much radiation would a person's eye, hand, testicle, stomach, etc be exposed to during such a failure.
Which brings me to how the scanner works. Essentially, it appears that an X-ray beam is rastered across the body, which highlights the importance of one of the specific concerns raised by the UCSF scientists... what happens if the machine fails, or gets stuck, during a raster. How much radiation would a person's eye, hand, testicle, stomach, etc be exposed to during such a failure.What is the failure rate of these machines?
What is the failure rate in an operational environment?
Who services the machine? What is the decay rate of the filter?
What is the decay rate of the shielding material?
What is the variability in the power of the X-ray source during the manufacturing process?
This last question may seem trivial; however, the Johns Hopkins Applied Physics Laboratory noted significant differences in their test models, which were supposed to be precisely up to spec.
It's also interesting to note that the Johns Hopkins Applied Physics Laboratory criticized other reports from NIST (the National Institute of Standards and Technology) and a group called Medical and Health Physics Consulting for testing the machine while one of the two X-ray sources was disabled (citations at the bottom of the page). These questions have not been answered to any satisfaction and the UCSF scientists, all esteemed in their fields and members of the National Academy of Sciences have been dismissed based on a couple of reports seemingly hastily put together by mid-level government lab technicians.
The documents that I have reviewed thus far either have NO AUTHOR CREDITS or are NOT authored by anyone with either a Ph.D. or a M.D., raising serious concerns of the extent of the expertise of the individuals and organizations evaluating these machines. Yet, the FDA and TSA continue to dismiss some of the most talented scientists in the country...
With respect to errors in the safety reports and/or misleading information about them, the statement that one scan is equivalent to 2-3 minutes of your flight is VERY misleading. Most cosmic radiation is composed of high energy particles that passes right through our body, the plane and even most of the earth itself without being absorbed or even detected. The spectrum that is dangerous is known as ionizing radiation and most of that is absorbed by the hull of the airplane. So relating non-absorbing cosmic radiation to tissue absorbing man-made radiation is simply misleading and wrong.
Furthermore, when making this comparison, the TSA and FDA are calculating that the dose is absorbed throughout the body. According the simulations performed by NIST, the relative absorption of the radiation is ~20-35-fold higher in the skin, breast, testes and thymus than the brain, or 7-12-fold higher than bone marrow. So a total body dose is misleading, because there is differential absorption in some tissues.
Of particular concern is radiation exposure to the testes, which could result in infertility or birth defects, and breasts for women who might carry a BRCA1 or BRCA2 mutation. Even more alarming is that because the radiation energy is the same for all adults, children or infants, the relative absorbed dose is twice as high for small children and infants because they have a smaller body mass (both total and tissue specific) to distribute the dose. Alarmingly, the radiation dose to an infant's testes and skeleton is 60-fold higher than the absorbed dose to an adult brain!
There also appears to be unit conversion error in the Appendix of the report, which was recently cited by the FDA in response to the UCSF scientist's letter of concern, which might mean that the relative skin dose is 1000-fold higher than the report indicates (pg Appendix B, pg ii, units of microSv are used in an example calculation, when it appears that units of milliSv should have been used).
I attempted to contact the author, Frank Cerra, to query whether this was a computational mistake or an unexplained conversion; however, none of his web-published email addresses are valid and there was no answer by phone. I cannot rule out that a conversion factor was used that was not described in the methods, and would welcome confirmation or rebuttal of this observation.
Finally, I would like to comment on the safety of the TSA officers (TSO) who will be operating these machines, and will be constant 'bystanders' with respect to the radiation exposure. The range of exposure estimates is a function of where an officer stands during their duty, what percentage of that duty is spent in the same location and how often the machine is running. A TSO could be exposed to as much as 86-1408 mrem per year (assuming 8 hours per day, 40 hours a week, 50 weeks per year and between 30-100% duty and 25-100% occupancy, as defined by the Johns Hopkins report), which is between 86%-1410% of the safe exposure of 100 mrem.
At the high end, if for example a TSO is standing at the entrance of the scanner when it is running at maximum capacity, then that officer could hit their radiation exposure limit in as few as 20 working days (assuming an 8 hour shift). While we may not be very happy with our TSOs at the moment as the face of these policies, we need to keep in mind that they really should be wearing radiation badges in order to know their specific exposure (especially for those officers who may also have to receive radiation exposure for medical reasons).
As far as I'm concerned, the jury is still out on whether these machines are safe or even could be made safe for this application. Until then, I suggest keeping your family out of these machines and as vile as it is, either submit to a physical search or just don't fly. Safety reports that should be considered invalid due to the fact that one of the two X-ray sources was disabled during testing:
- Medical and Health Physics Consulting, Radiation Report on Rapiscan Systems Secure 1000 (March 21, 2006).
- Medical and Health Physics Consulting, Radiation Report on Rapiscan Systems Secure 1000 (June 5, 2008).
- Medical and Health Physics Consulting, Supplement to Report dated June 5, 2008 (October 28, 2008).
- National Institute of Standards and Technology Assessment of Radiation Safety and Compliance with ANSI N43.17-2002 Rapiscan Dual Secure 1000 Personnel Scanner (July 9, 2008).
UPDATE
Just to clarify, I am not a radiation biologist, radiologist, health physicist, etc... my expertise is actually in single molecule biophysics and the biochemistry of DNA repair. This article is simply my review of the safety reports published by the TSA on their website, and not the result of any independent evaluation or experimentation. Also, all views and comments are my opinion (professional and unprofessional) and are not endorsed or representative of the University of California or any affiliated departments or colleges.
Which brings me to how the scanner works. Essentially, it appears that an X-ray beam is rastered across the body, which highlights the importance of one of the specific concerns raised by the UCSF scientists... what happens if the machine fails, or gets stuck, during a raster. How much radiation would a person's eye, hand, testicle, stomach, etc be exposed to during such a failure.
What is the failure rate of these machines?
|What is the failure rate in an operational environment?
Who services the machine?
What is the decay rate of the filter?
What is the decay rate of the shielding material?
What is the variability in the power of the X-ray source during the manufacturing process?
This last question may seem trivial; however, the Johns Hopkins Applied Physics Laboratory noted significant differences in their test models, which were supposed to be precisely up to spec. Its also interesting to note that the Johns Hopkins Applied Physics Laboratory criticized other reports from NIST (the National Institute of Standards and Technology) and a group called Medical and Health Physics Consulting for testing the machine while one of the two X-ray sources was disabled (citations at the bottom of the page).
These questions have not been answered to any satisfaction and the UCSF scientists, all esteemed in their fields and members of the National Academy of Sciences have been dismissed based on a couple of reports seemingly hastily put together by mid-level government lab technicians.
The documents that I have reviewed thus far either have NO AUTHOR CREDITS or are NOT authored by anyone with either a Ph.D. or a M.D., raising serious concerns of the extent of the expertise of the individuals and organizations evaluating these machines. Yet, the FDA and TSA continue to dismiss some of the most talented scientists in the country...Furthermore, when making this comparison, the TSA and FDA are calculating that the dose is absorbed throughout the body. According the simulations performed by NIST, the relative absorption of the radiation is ~20-35-fold higher in the skin, breast, testes and thymus than the brain, or 7-12-fold higher than bone marrow. So a total body dose is misleading, because there is differential absorption in some tissues.
Of particular concern is radiation exposure to the testes, which could result in infertility or birth defects, and breasts for women who might carry a BRCA1 or BRCA2 mutation. Even more alarming is that because the radiation energy is the same for all adults, children or infants, the relative absorbed dose is twice as high for small children and infants because they have a smaller body mass (both total and tissue specific) to distribute the dose. Alarmingly, the radiation dose to an infant's testes and skeleton is 60-fold higher than the absorbed dose to an adult brain!
3 comments :
Wow. Great article!
Good article, generally well thought out and factual. I'd lose the pictures that have nothing to do with the content.
Also, the amount of radiation needed to cause sterility is very high and not a consideration here.
Very informative and impressive post you have written, this is quite interesting and i have went through it completely, an upgraded information is shared, keep sharing such valuable information. Digital X Ray Centres in Secunderabad
Post a Comment